Two Humanoid Robots Removed an Organ From a Living Animal, but They Were Not Acting Alone
Humanoid robots have completed gallbladder surgery on live pigs for the first time. The milestone could reshape access to surgery, but every movement was still controlled by human surgeons.
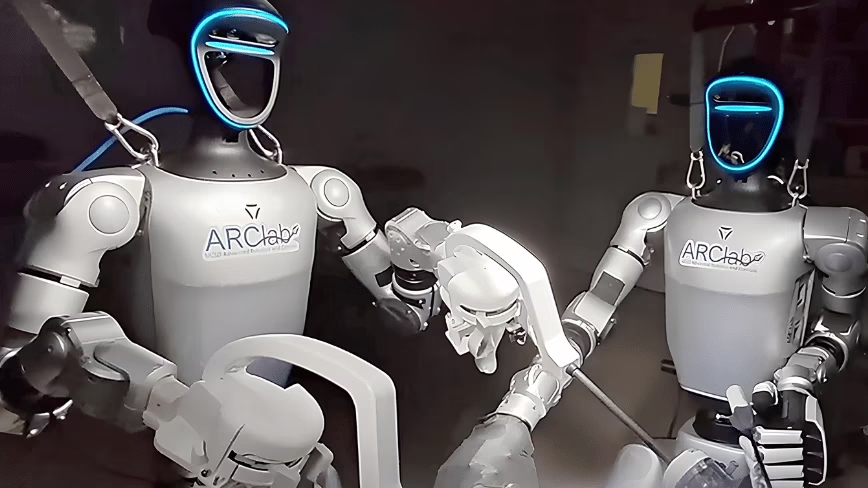
Two humanoid robots have crossed a boundary that, until now, belonged mainly to purpose-built surgical machines. In a preclinical study at the University of California San Diego, modified commercial robots performed minimally invasive gallbladder operations on living pigs.
The result is visually striking: a machine shaped like a person stands beside an operating table, grips standard laparoscopic instruments and works inside a living body. Yet the most important detail is also the easiest to miss. These robots were not autonomous surgeons. Human doctors controlled every surgical movement.
What the researchers achieved
The team adapted Unitree G1 humanoid robots for laparoscopic surgery and evaluated them through benchtop tests, simulated surgical exercises and two procedures on live pigs. The study was published in Nature as an in vivo feasibility assessment of humanoid robots in surgery.
Both procedures were laparoscopic cholecystectomies, the medical term for removing the gallbladder through small incisions. The robots participated in the central steps of the operation, including retracting tissue, dissecting around the gallbladder, applying clips and separating the organ from the liver bed.
The researchers tested two configurations:
- In the first procedure, one humanoid robot acted as the primary operator while a human surgeon assisted beside the table.
- In the second, two humanoid robots worked side by side and handled the surgical instruments, while human surgeons controlled both machines remotely.
The procedures demonstrated that a general-purpose humanoid platform can manipulate conventional laparoscopic tools during a complex operation on living tissue. That is the core breakthrough. It is a proof of physical and technical feasibility, not proof of independent robotic judgment.
How the robotic surgery system worked
Surgeons remained in control
The system used teleoperation. A surgeon sat at a control station and moved hand controllers while viewing the surgical field. Software translated those movements into commands for the robot's arms and the instruments inside the animal.
This setup resembles the control principle behind established robotic surgery systems, but the machine at the operating table is different. Conventional platforms are engineered specifically for surgery and often use fixed arms positioned around the patient. The experimental system placed surgical tools in the hands of a mobile humanoid body.
The distinction between teleoperation and autonomy is critical. The robots did not decide where to cut, identify complications independently or determine the correct clinical response. The surgeon remained responsible for perception, judgment and action. The robot served as a physical surrogate.
Commercial hardware was modified
The Unitree G1 was not designed for an operating room. Researchers added interfaces that allowed it to hold standard laparoscopic instruments and created a control framework that mapped the operator's motions onto the robot.
Using commercially available hardware matters because it tests whether a general-purpose machine can enter an environment designed for people without requiring the entire room to be rebuilt around it. It also creates a path for researchers to improve software and surgical attachments without developing every mechanical component from zero.
Why a humanoid body could matter
Hospitals, operating rooms, doors, work surfaces and medical tools are designed around the dimensions and movements of the human body. A humanoid robot could potentially fit into those spaces, use existing equipment and move between different duties.
A specialized surgical platform may outperform a humanoid at a single procedure. The proposed advantage of a humanoid is versatility. In theory, one machine could prepare equipment, position a camera, assist a surgeon, move supplies and later support other physical tasks in the hospital.
That versatility could become valuable in locations where expertise and equipment are scarce. Possible settings include:
- Rural or remote hospitals without permanent access to specialist surgeons.
- Disaster zones where local medical infrastructure has been damaged.
- Ships, offshore facilities and isolated research stations.
- Military field hospitals where specialists cannot safely travel.
- Future space missions where evacuation or rapid specialist deployment is impossible.
In such settings, a specialist might control the robot from another location. The medical expertise would remain human, but the robot could provide a body through which that expertise reaches the patient.
What the study does not prove
The experiment does not show that humanoid robots are ready to operate on people. It also does not establish that they are safer, faster or more effective than mature surgical systems.
The research identified significant technical limitations. The humanoid platform was slower during surgical tasks, had a shorter effective reach and experienced control delays. The team also needed pauses and recalibration during the operations.
These are not minor inconveniences in a clinical environment. A delay of a fraction of a second, an unexpected joint movement or a loss of precision can matter when instruments are close to blood vessels and delicate tissue.
Precision, speed and latency
Established surgical robots are designed to filter tremor, scale motion and maintain stable instrument geometry. A general-purpose humanoid must balance many competing requirements, including mobility, reach, strength and compactness. Surgical precision is only one of them.
Communication latency is another obstacle. Remote surgery requires the robot to respond quickly and predictably to the surgeon's commands. Delays can make precise movements harder and may become more serious when the operator and robot are separated by long distances or unreliable networks.
Safety and regulation
Before any human use, a system like this would require extensive reliability testing, sterilization procedures, failure recovery mechanisms and regulatory review. Researchers would need to show what happens if a motor stalls, a network connection drops, a sensor gives an incorrect reading or the robot loses power during a procedure.
The experiment was conducted on pigs as a preclinical feasibility study. Moving from that setting to human trials would require a much larger body of evidence and carefully controlled development.
Autonomy is a separate question
Humanoid appearance can encourage people to assume human-like intelligence. In this study, the body was humanoid, but the surgical agency remained with the doctors.
Future systems may automate bounded tasks such as holding a camera steady, passing an instrument, positioning equipment or maintaining a safe viewing angle. Those functions could reduce workload without transferring the entire operation to artificial intelligence.
Full surgical autonomy would raise harder technical and ethical questions. A machine would need to recognize unusual anatomy, respond to bleeding, understand when a plan should change and know when to stop. It would also require clear rules for responsibility when software, hardware, communications and clinical decisions interact.
What happens next
The immediate research challenge is not replacing surgeons. It is improving the platform until it can match the stability, responsiveness and precision expected from medical equipment.
Likely next steps include reducing latency, extending reach, improving force control, adding stronger safety constraints and testing a broader range of tasks. Researchers will also need direct comparisons with specialist surgical systems to determine where a humanoid offers a real advantage.
The strongest case may ultimately be broader than surgery. A humanoid that can perform many useful hospital duties and occasionally serve as a teleoperated surgical assistant could justify its general-purpose form more convincingly than a machine used only for operations.
The bigger picture
This study offers a glimpse of remote medicine, not an autonomous robotic doctor. It shows that a commercial humanoid can be adapted to perform demanding surgical motions on living tissue while controlled by trained professionals.
For now, the surgeon still observes, decides and operates. The robot supplies a new physical presence. If engineers can make that presence reliable, precise and safe, specialist care could eventually reach places where the specialist cannot.
Sources and citations
Published by
NewTaqnia Editorial
Technology & innovation desk